26 August 1977; revised 4 October 1977 0036-8075/78/0707-0079$00.50/0
Home » Anxiety Change Through Electroencephalographic Alpha Feedback Seen Only In High Anxiety Subjects
James V. Hardt and Joe Kamiya
Science, Vol. 201, pp. 79-81, 7 July 1978
Subjects who were either high or low in trait anxiety used alpha feedback to increase and to decrease their electroencephalographic alpha activity. The alpha changes were tightly linked to anxiety changes, but only in high anxiety subjects (for whom anxiety was reduced in proportion to alpha increases, and was increased in proportion to alpha suppression). Low trait-anxiety subjects were superior at both enhancement and suppression training, but their alpha changes were not related to anxiety changes. In both groups, anxiety changes were generally unrelated to either resting levels or changes in frontalis electromyograms and respiration rate. These results suggest that long-term alpha feedback training (at least 5 hours) may be useful in anxiety therapy.
Recently, Orne and Paskewitz (1) reported “a lack of the expected relationship between alpha density and the apprehension, anxiety, fear, or arousal level of the subjects” (1, p. 460). This paradoxical outcome, counter to 35 years of electroencephalographic (EEG) research (2), was interpreted to cast doubt on the “expected” inverse alpha anxiety relationship, and to “challenge the widely accepted rationale for using alpha feedback training as a means of teaching individuals control … of anxiety.”
However, several methodological problems and unproved assumptions weaken their challenge to the use of learned alpha increases for anxiety. Ome and Paskewitz (1) did not select high anxiety subjects; in fact they probably eliminated them by excluding subjects with low alpha levels and subjects afraid of electric shock. Instead, they sought to increase anxiety (by threat of electric shock) and then to measure alpha changes. Anxiety levels were never directly measured and no attempt was made to measure alpha changes accompanying reduced anxiety. Orne and Paskewitz reasoned backward from their anxiety manipulations to conclusions about possible effects of alpha manipulations (that is, through feedback). Their reasoning assumed a symmetric relation between alpha activity and anxiety. However, nonsymmetric relations are common. Thus (absent symmetry) shock-induced increases in anxiety could fail to affect alpha as reported (1) and yet feedback-induced alpha increases could still effect anxiety reductions.
The problem in anxiety therapy is to reduce, not increase, anxiety, so we trained both high and low trait-anxiety people to control the amount of alpha activity (8 to 13 Hz) in their brain waves. Occurrence of EEG alpha activity sounded a tone whose loudness was proportional to the instantaneous alpha voltage. Volunteers for alpha feedback training (100 college males) were paid $1.50 USD to take the Minnesota Multiphasic Personality Inventory (MMPI). Selection of the eight subjects with the highest trait anxiety, and eight subjects with the lowest trait anxiety was based on the MMPI’s Welsh A (anxiety) scale and the MMPI’s three validity scales (3). The resultant high and low trait-anxiety groups had average Welsh A anxiety scores (27.4 and 4.3, respectively) which differed reliably (P < .05 considered reliable). The full MMPI was given two more times. After one day on which alpha baseline data (no feedback) were obtained, subjects took MMPI No. 2 and then trained for seven consecutive days on alpha feedback, after which MMPI No. 3 was given. Subjects were paid $2.50 USD per day.
TABLE 1 CORRELATION OF TRAIT-ANXIETY CHANGE WITH PHYSIOLOGICAL CHANGES DURING ALPHA ENHANCEMENT FEEDBACK. PHYSIOLOGICAL CHANGES WERE SUMMED ACROSS DAYS 4 TO 7 TO DERIVE THE NET PHYSIOLOGICAL CHANGES.
| Physiological Measure | Correlation in low anxiety subjects (N = 8) | Correlation in high anxiety subjects (N = 8) |
|---|---|---|
| sum Oz alpha | .291 | -.767 (P < .025) |
| per cent O1, alpha | .242 | -.933 (P < .001) |
| sum O1, alpha | .175 | -.697 (P < .05) |
| per cent C3 alpha | .247 | -.581 |
| sum C3 alpha | .413 | -.672 (P < .05) |
| Respiration rate | -.145 | -.319 |
| sum Frontalis EMG | .385 | -.558 |
Each day we recorded from each subject (i) mood scales, (ii) an 8-minute resting baseline, (iii) 32 minutes of alpha enhancement feedback, (iv) mood scales, (v) an 8-minute resting baseline, (vi) 16 minutes of alpha suppression feedback, and (vii) mood scales. Subjects sat erect, eyes closed, in total darkness for all recording. Mood scales included the “state” form of the Multiple Affect Adjective Check List (MAACL) to measure changes in state anxiety during feedback. State anxiety is a short-term feeling of the moment. Trait anxiety refers to a longer-term personality disposition. The MAACL measure of state anxiety correlates significantly with other anxiety measures: clinical, situational, physiological, and biochemical (4). Alpha activity was measured at three sites: Oz (midline occipital), O1 (left occipital), and C3 (left central) (linked ears were used for reference). Integrated amplitude (sum) scores were derived from all three sites, and percentage time scores (10 micro-volt threshold) were derived from O1 and C3. The percentage scores are questionable statistically (5), but are included for comparisons (1). Feedback was a tone (loudness proportional to Oz alpha amplitude) and a digital score representing summed Oz alpha, presented at 2-minute intervals. Frontalis muscle tension was also scored [integrated electromyogram (EMG)], and abdominal respiration was recorded.
To test the data as a single dependent variable representing the alpha/anxiety relation, we paired each individual’s daily alpha changes (during enhancement or suppression) with his resultant state-anxiety changes. These paired values were then correlated across subjects (separately in each trait-anxiety group). Significant negative correlations would confirm an inverse alpha / anxiety relation. To test for this, Bartlett’s (6) method was used: alpha / state-anxiety correlations from each of the 7 days of feedback were z-transformed and tested across days with analysis of variance (ANOVA). State-anxiety changes were related to EMG and respiration rate changes the same way. Trait-anxiety changes were also treated separately in each group, being correlated with cumulative (net) alpha changes during enhancement or suppression. Net alpha change across days best indexes amount of exposure to anxiety-altering states. Trait-anxiety change was the Welsh A difference between MMPI Nos. 1 and 3 (given before and after the seven feedback sessions). Net alpha change (7-10) was the sum of daily alpha changes (feedback minus prior baseline). Net EMG and respiration rate changes were determined similarly.
Alpha enhancement reliably reduced state anxiety in the high trait-anxiety group. The inverse relation (seen with all five alpha measures) was significant with both f and percentage measures of C, alpha. The inverse relation was “complete” in that alpha suppression increased state anxiety. This effect (seen with all five alpha measures) was significant with all measures of occipital alpha: sum Oz, sum O1, percentage O1. The negative relation linking alpha increases to reduced state anxiety became stronger as high trait-anxiety subjects trained beyond 2 hours (see Fig. 1). Despite the full range of effects in the high trait-anxiety subjects, low trait-anxiety subjects showed no significant alpha/state-anxiety effects.
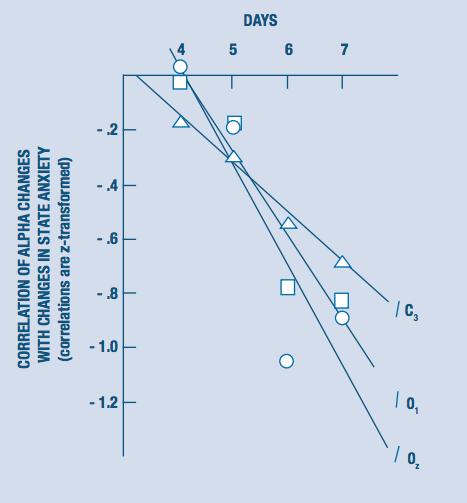
FIGURE 1 THE CORRELATION (Z-TRANSFORMED) BETWEEN ALPHA CHANGE AND STATE-ANXIETY CHANGE AS A FUNCTION OF TRAINING TIME AND CORTICAL SITE. THE CORRELATIONS WERE DERIVED FROM STATE-ANXIETY CHANGES OF EIGHT HIGH ANXIETY SUBJECTS DURING ALPHA ENHANCEMENT, AND FROM THE INTEGRATED AMPLITUDE ALPHA SCORES OF THESE SUBJECTS AT THREE CORTICAL SITES: 0Z (D), 01 (F–L), AND C3 (A). AFTER EACH OF THE FOUR INDICATED DAYS (4, 5, 6, AND 7) THE TOTAL ACCUMULATED FEEDBACK TRAINING TIME (IN MINUTES) WAS 176, 224, 272, AND 320. LINEAR REGRESSIONS OF Z SCORES ON DAYS WERE SIGNIFICANT AT TWO OF THE THREE CORTICAL SITES. THE COEFFICIENT OF DETERMINATION (RL) WAS .791, .896, AND .987 FOR, RESPECTIVELY, SUM OZ, SUM O1, AND SUM C3 ALPHA SCORES. THUS, AS TRAINING PROGRESSED, ALPHA ENHANCEMENT BECAME MORE RELIABLY ASSOCIATED WITH STATE ANXIETY REDUCTIONS.
Alpha enhancement also reduced the (supposedly stable) Welsh A trait anxiety measure. The key finding (see Table 1) was that net alpha increase (7) was related to trait-anxiety decrease only in high trait-anxiety subjects. Reductions in trait anxiety were large enough to be useful in anxiety therapy. The two best alpha enhancers in the high anxiety group reduced their Welsh A scores from 35 and 24 (before feedback) to 18 and 7, respectively (after feedback). This left both below average in anxiety. These trait-anxiety changes followed substantial net increases in alpha activity, relative to baselines (see Table 2). Net alpha suppression had no significant effect on trait anxiety for either anxiety group, perhaps because daily suppression practice lasted only half as long as enhancement (16 as opposed to 32 minutes). No respiration effects were seen and the only EMG effect was in low trait anxiety subjects who showed a direct relation between EMG and state anxiety during the alpha suppression task.
Relating trait-anxiety change to net alpha change for each individual insulated these results against regression to the mean; nevertheless corrections for such regression were made (11-14). Results remained significant. Even reanalysis with another MMPI anxiety scale (Taylor Manifest Anxiety) gave confirmation: alpha increases led to trait-anxiety reductions in high (but not low) trait-anxiety subjects. Several other results may aid interpretation. Low trait-anxiety subjects enhanced and suppressed alpha better than high trait-anxiety subjects, as shown previously (15). Daily alpha baselines were stable across days, and low anxiety subjects tended to have higher baselines at C3. However these baseline differences did not reach significance [F(6, 84) = 2.02, P < .08, and F(6, 84) = 1.41, P < .25, for percentage and sum measures, respectively]. The measurement equipment was both sensitive and accurate, being capable of resolving differences of half a microvolt sustained over 2 minutes. Variances with a 10-Hz, 50-microV input were less than 1 percent of the means.
TABLE 2 ALPHA ENHANCEMENT INDICES FOR THE TWO BEST HIGH ANXIETY SUBJECTS (R.L. AND G.W.). THE LARGE PERCENTAGE INCREASES IN PERCENTAGE TIME SCORES OCCUR WHEN SUBJECTS START NEAR THE THRESHOLD (HERE 10 GV). AN INCREASE FROM 5 TO 50 PERCENT TIME ALPHA IS A 1000 PERCENT INCREASE. INCREASES FOR R.L. AND G.W. WERE AVERAGED TOGETHER ACROSS THE LAST 4 DAYS OF TRAINING (DAYS 4 TO 7).
| Average Physiological Measure | Daily peak enhancement (percentage above average baseline)1 | Alpha score (percentage above daily baseline)2 |
|---|---|---|
| sum Oz | 18 | 95 |
| percent Oz | 40 | 192 |
| sum O1 | 21 | 98 |
| percent O1 | 128 | 1000 |
| sum C3 | 16 | 49 |
TABLE NOTE 1: THESE REPRESENT ALPHA INCREASES SUSTAINED FOR MORE THAN 2 HOURS (4 DAYS OF TRAINING AT 32 MINUTES OF ENHANCEMENT PER DAY, OR 128 MINUTES). TABLE NOTE 2: DAILY PEAK ENHANCEMENT SCORES FOR THE HIGHEST 2-MINUTE SCORING INTERVAL WERE COMPARED WITH AVERAGE DAILY BASELINES, AND THE PERCENTAGE INCREASES WERE AVERAGED ACROSS DAYS 4 TO 7.
Stability of these alpha/anxiety findings across a variety of methods of representing changes (11, 16) affirms the classical inverse alpha/anxiety relation, but only in high trait-anxiety subjects, for whom the classical relation is “complete.” Alpha increases result in state-anxiety decreases, while alpha decreases result in state-anxiety increases. This “completeness” implies that anxiety decreases during enhancement do not result from feelings of success, since success at suppression yields anxiety increases. Our data nowhere suggest factors other than alpha changes producing the anxiety changes. Permanence of anxiety changes requires assessment. Preliminary evidence (17) suggests poor enhancement in high anxiety subjects is associated with rapid baseline respiration. Prior training in slow breathing may facilitate alpha enhancement and anxiety reduction in such persons.
Absence of alpha/anxiety effects in low trait-anxiety subjects explains why Ome and Paskewitz (1) observed no inverse alpha/anxiety relation: they eliminated 60 percent of their original subjects in two successive screenings, leaving a possibly low trait-anxiety group. Subjects showing alpha activity less than 25 percent of the time were excluded first. Such subjects are often high in trait anxiety (2). Remaining subjects were asked to volunteer for “painful” electric shock. Over half withdrew. The ten remaining volunteers were probably low in trait anxiety (18), and gave Ome and Paskewitz negative results which agree perfectly with our results for low anxiety subjects. But, in addition, we report positive results in high trait-anxiety subjects. The relation between alpha enhancement and reduced state anxiety was seen centrally at C3, while alpha suppression at occipital sites (Oz, O1) was related to anxiety increases. This difference indicates a complex relation between alpha location and state-anxiety changes. It may explain disagreements between studies, and suggests existence of a best feedback site for reducing state anxiety. However, alpha increases at all three sites were related to reduction of trait anxiety (Table 1), whereas EMG’s were unrelated to changes in either state or trait anxiety (in high trait-anxiety subjects). Thus alpha feedback may be a more effective treatment for high anxiety than EMG feedback.
Malmo’s (19) description of an inverted U-shaped relation between alpha and arousal correctly predicts the signs of the alpha/anxiety relation for high and low anxiety subjects if, like Ome and Paskewitz, we equate anxiety and arousal (see Table 1). Low-arousal people must become more aroused to increase alpha, while over-aroused people must learn reduced arousal. This learning takes time and data obtained during the first 2 hours are best discarded. Our results suggest the possibility that alpha feedback can be used therapeutically, but to obtain therapeutic effects more extended training should be given than that reported in most studies.
JAMES V. HARDT, JOE KAMIYA
Langley Porter Neuropsychiatric Institute, University of California, San Francisco 94143
26 August 1977; revised 4 October 1977 0036-8075/78/0707-0079$00.50/0
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking "Accept", or continuing to use this website, you consent to our use of ALL cookies. For more information on how we use cookies, please review our Privacy Policy.

Get your FREE copy now!